 DONATE NOW
DONATE NOWPreventing Angle-Closure Glaucoma
Doctors perform laser iridotomy for glaucoma to prevent damage caused by angle-closure glaucoma. Angle-closure glaucoma can have a sudden, painful onset or result in deterioration of your vision over time. Laser iridotomy prevents angle closure glaucoma.
What is a Laser Iridotomy?
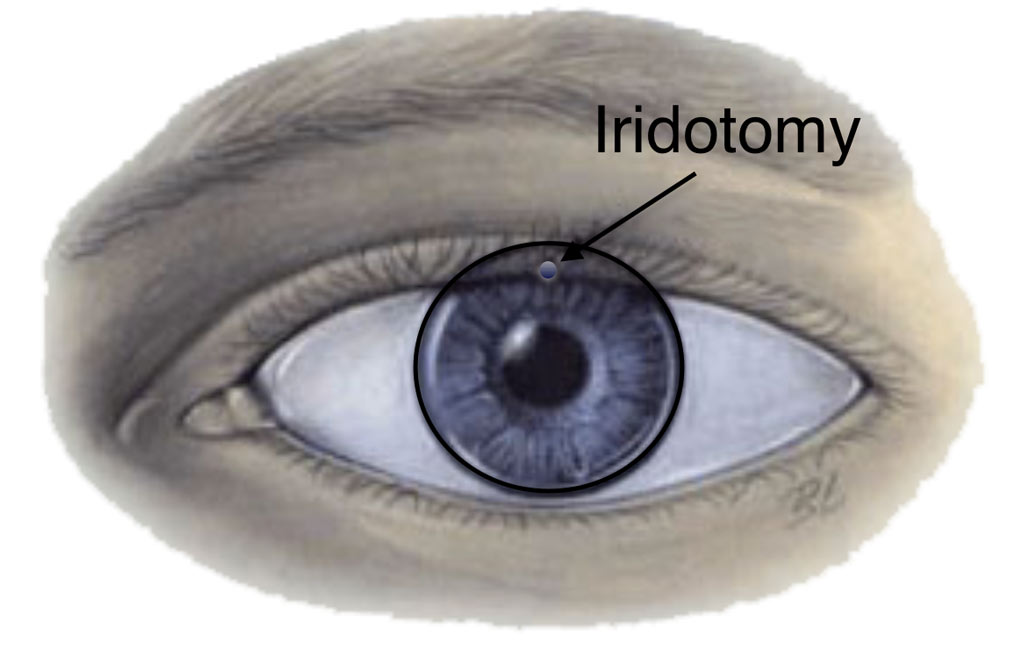
Closed-angle (of pupillary-block) glaucoma is one of many types of glaucoma. Doctors often cure closed-angle glaucoma with a procedure called iridotomy. To understand this treatment, it is important to know the factors that determine eye pressure. During laser iridotomy, doctors create a small hole in the iris, the colored part of the eye. They usually place the iridotomy in the upper iris, hidden under the upper eyelid.
What is Eye Pressure?
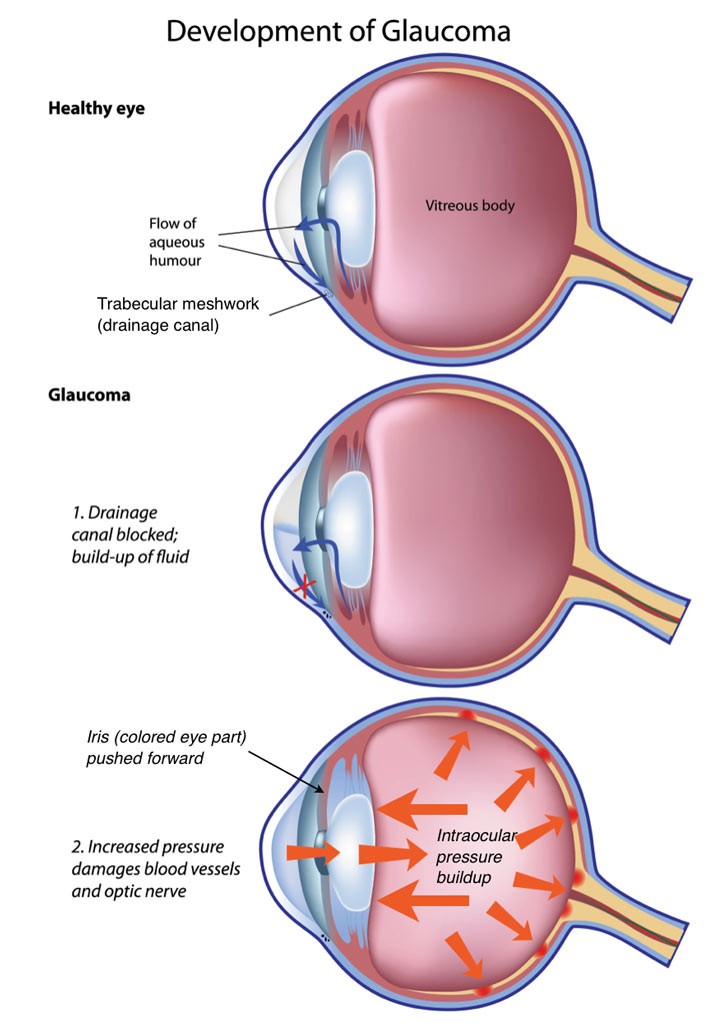
Aqueous humor (the nourishing fluid within the front of the eye) leaves the eye through a tiny drain called the trabecular meshwork.
Aqueous humor leaves the eye through a tiny drain called the trabecular meshwork, which is located just in front of the iris.
The trabecular meshwork is located on the side of the eye, just in front of the iris (the part which gives an eye color). Since the ciliary body produces fluid just behind the iris, it flows between the iris and lens before exiting through the trabecular meshwork.
In the normal eye, fluid passes between the iris and lens before leaving through the trabecular meshwork in the front of the eye.
In pupillary-block glaucoma, a type of closed-angle glaucoma, fluid cannot flow between the iris and lens, causing eye pressure to rise. As pressure increases, it pushes the iris forward.
The eye’s pressure depends on the balance between fluid production and drainage. All eyes have measurable pressure. When the eye drains less aqueous humor, pressure rises, often leading to glaucoma.
Although many people think of glaucoma as just one single disease, in fact there are many different forms of glaucoma. Differences depend upon where in the eye the blockage to the drainage occurs. The iris-lens border and the trabecular meshwork can both limit aqueous flow, increasing eye pressure. Pupillary-block glaucoma occurs at the iris-lens border. In this type of closed-angle glaucoma, fluid cannot pass between the iris and lens. Doctors call it pupillary-block glaucoma because fluid gets trapped behind the pupil.
As many as 10% of all glaucoma patients in the United States may have pupillary-block glaucoma. The blockage of fluid flow between the iris and lens can cause the pressure behind the iris to rise. The rising pressure pushes the iris forward. If it moves forward enough, the iris can cover trabecular meshwork like a rubber stopper in a drain. Sometimes a patient is unaware of the pupillary-block. However, the eye may become red. A patient also may experience headache or pain, blurred vision, and halos around lights. Rarely, there is nausea.
If sudden pupillary-block occurs and the eye remains untreated, permanent damage can cause blindness. Treating the fluid blockage between the iris and lens quickly reduces damage. Therefore, it is desirable to treat this disease as early as possible.
Laser Iridotomy
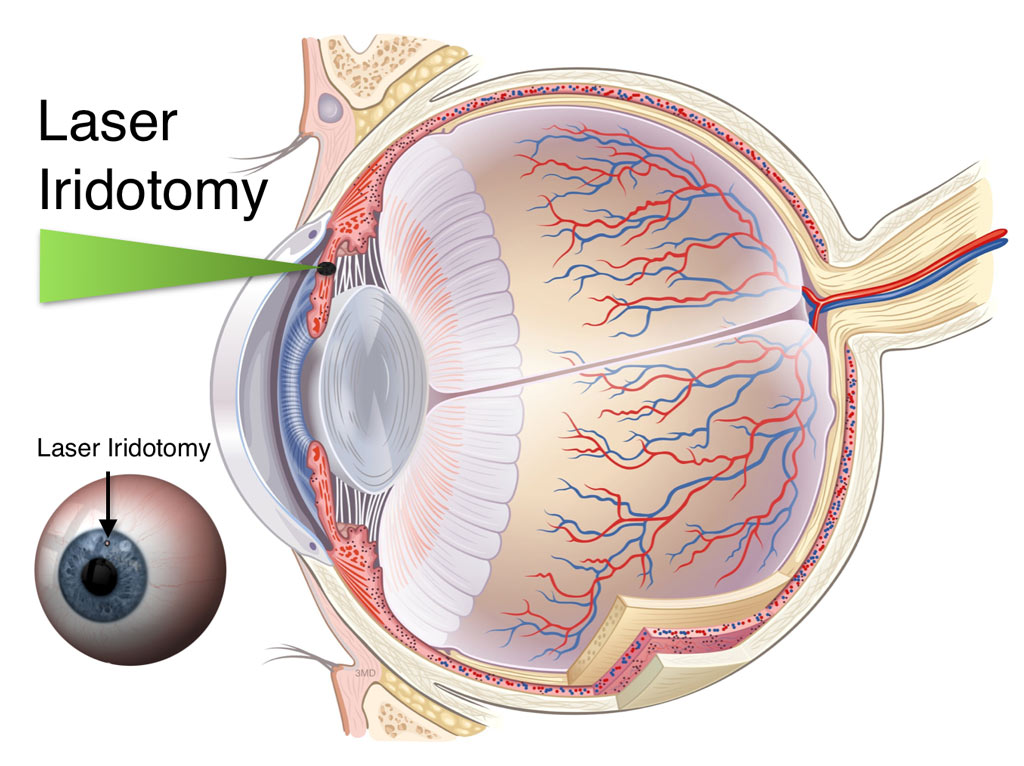
The best treatment for pupillary-block glaucoma is to create a hole in the iris (known as an iridotomy). The iridotomy restores the flow of fluid to the front of the eye by bypassing the pupil, the site of the blockage. This small hole in the iris releases pressure in the eye. Once fluid passes through the iridotomy, the iris no longer pushes forward. Fluid can leave the eye through the trabecular meshwork again.
How do Lasers Work to Treat Glaucoma?
Lasers deliver a type of light energy. This type of light energy is similar to using a magnifying glass to harness the energy of the sun to burn a hole in a piece of paper on a sunny day. The magnifying glass needs to properly focus the light to create a hole in the paper. Similarly, the laser has no effect if doctors do not aim it properly at the iris. In order to focus the laser, your eye doctor uses an instrument called a slit-lamp.
Doctors use the same instrument to examine your eyes routinely. Since this instrument acts as a microscope, it focuses the laser energy with extreme accuracy.
Doctors can use several types of lasers to treat pupillary-block glaucoma. By 1980, ophthalmologists widely used the argon laser to create an iridotomy. Since then, studies have shown that the neodymium: YAG laser also works safely and effectively. Although these lasers differ in some ways, your ophthalmologist will decide which one to use.
How do Doctors Perform Laser Iridotomy?
Before having an iridotomy, your ophthalmologist may place some different types of drops on your eye. The first drop, pilocarpine, will make your pupil smaller. This stretches and thins your iris, similar to stretching out the top surface of a drum. By doing this, it is easier for the laser to penetrate and make a hole in your iris. Your doctor may ask you to continue using this eye drop for a few days after the laser treatment. This medication may temporarily cause blurred vision (especially at night) and also may give you a brow-ache.
Your doctor may use another type of eye drop within a few hours of laser treatment to prevent or treat increased eye pressure. Additionally, they may use other drops to reduce inflammation.
Anesthesia Eye Drops
The only kind of anesthesia required to perform a laser iridotomy is an eye drop. This is the same type of drop your doctor uses to measure your eye pressure. With the eye drop, the laser surgery should be painless. You may see a bright light, like a photographer’s flash from a close distance. Also, you may feel a pinch-like sensation.
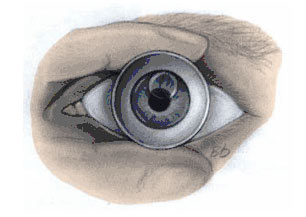
Your doctor will next place a special contact lens on your eye to focus the laser light upon the iris. This lens keeps your eyelids separated so that you do not blink during the treatment. This also reduces small eye movements so that you do not have to worry about your eye moving during the treatment. Doctors place special jelly on the contact lens to protect the eye from scratches. This jelly may remain on your eye for about 30 minutes, leading to blurred vision or a feeling of heaviness.

What to Expect After an Iridotomy
After treatment, your doctor may ask you to stay for a few hours to check your eye pressure and insure that it has not increased.
When it is safe, your doctor will send you home and ask you to use eye drops. Your ophthalmologist will explain how to use them and when to return for a follow-up exam.
In general, there are no restrictions in activity following the laser treatment. You can return to your normal daily chores immediately. It is advisable to have someone drive you home from your doctor’s office. You can expect some redness of the eye, a sensitivity to light, and a scratchy sensation. All of these might last for a period of days. You also might expect a small headache later that day or night.
The chance of losing vision following a laser procedure is extremely small. The main risks of a laser iridotomy are that your iris might be difficult to penetrate, requiring more than one treatment session. The other risk is that the hole in your iris will close. This happens less than one-third of the time. Once the hole stays open for six weeks, it is unlikely that it will close in the future. In addition, you may still require medications, or other treatments to keep your eye pressure sufficiently low. This further treatment is necessary if there is damage to the trabecular meshwork prior to the iridotomy or if you also have one of the other types of glaucoma, in addition to the pupillary-block type.
Do not worry about the size of the hole in your iris. Neither you nor your friends will notice it. Doctors usually place it in a portion of the iris covered by your upper eyelid. The size of the iridotomy is only that of a pin head.
Remember that the creation of a laser iridotomy is both safe and effective. There are a few risks. The purpose of an iridotomy is to preserve your vision, not to improve it.